This is the research blog of Dr Sally Pezaro. Dr Pezaro is working to secure excellence in perinatal services. Specialist interests include workforce, gender and midwifery research.
In the largest international study of it’s kind, we sought to uncover the qualities that make a midwife a strong leader, and how to cultivate those qualities within the profession. We surveyed hundreds of midwives and nurse-midwives from around the world (76 countries! … predominantly the United Kingdom (UK), Australia, the United States of America (USA), Canada, Uganda, Saudi Arabia, Tanzania, Rwanda, India, and Kenya. The results were enlightening.
What Makes a Strong Midwife Leader?
Midwives identified several key characteristics of strong leadership within their profession. These leaders were described as mediators, dedicated to their work, evidence-based practitioners, effective decision-makers, role models, advocates, visionaries, resilient, empathetic, and compassionate. These traits align with several established leadership styles, including compassionate, transformational, servant, authentic, and situational leadership.
How Can We Foster Strong Midwifery Leadership?
The study also explored ways to enable and strengthen midwifery leadership. Suggestions included investing in a clear professional identity for midwives, increasing societal recognition of the profession, ongoing research, leadership development opportunities, interprofessional collaboration, succession planning, and boosting midwives’ self-efficacy.
Why Does This Matter?
Midwifery is a crucial profession with a significant impact on perinatal health outcomes. By understanding and fostering strong leadership within midwifery, we can elevate the profession and improve perinatal care globally. The findings of this study can inform the development of new leadership models, frameworks, and tools for midwives, ultimately benefiting both practitioners and the families they serve.
This research sheds light on the complex and multifaceted nature of midwifery leadership, offering valuable insights for midwives, educators, and healthcare organizations seeking to cultivate strong leadership within the profession. By investing in midwifery leadership, we can create a brighter future for midwives and the communities they serve.
How do you thrive as a strong midwifery leader? Do you see strong leadership in others? Do you see this work being used as a framework to support midwifery leadership worldwide? – I would love to hear your thoughts.
Until next time…Look after yourselves and each other
It’s been an interesting start to the year with me appearing on the BBC Panorama ‘Midwives Under Pressure’ and BBC world news. You can watch the documentary via the QR code below.
This is of course an issue I feel very passionate about, and much of our research focusses upon the topics raised. It is hard and uncomfortable to talk about these issues, but nevertheless, we must continue to push forward. It is too important not to.
I received some backlash for appearing on the programme, but the majority of feedback was overwhelmingly positive. The programme itself generated much discussion about the issues raised, and I hope it also brought about some reflection in us all. There are always pushes and pulls in the media to take a certain angle on things. Nevertheless, its important we all move away from blame cultures and toward compassionate learning cultures in this.
I hear of negative consequences for healthcare workers speaking out, both through people who tell me their experiences and through the research we do. These issues were also raised on the programme. Whilst it is always important to speak out and escalate where we see concern, it is also important to avoid using referral to regulators as a threat, or making malicious allegations without genuine concern. It undermines the process and may cause harm. Thankfully, these kind of issues are recognised early and are often thrown out. Conversely, real concerns are often not heard when they need to be. Perhaps this is reflective of people’s need to protect reputations? in response to fear? a symptom of poor leadership? a result of toxic cultures?
There is certainly much to unpack here and we are working hard to secure change. What are your thoughts on this? I would love to hear more on this conversation.
Until next time…Look after yourselves and each other
Since publishing in Gender & Society, I have been invited to join some exciting projects and research/writing groups on the topic of gender diversity in midwifery. We are also recruiting a PhD project in this area. So expect more publications and outputs from these endeavours in due course.
Pezaro, S., Crowther, R., Pearce, G., Jowett, A., Godfrey-Isaacs, L., Samuels, I., & Valentine, V. (2023). Perinatal Care for Trans and Nonbinary People Birthing in Heteronormative “Maternity” Services: Experiences and Educational Needs of Professionals. Gender & Society, 37(1), 124–151. https://doi.org/10.1177/08912432221138086
My thinking and growth of understanding in this field is developing every day, and it’s exciting to think about what may come. For now, I wanted to share two things. One, a podcast I recorded with @DrAdamJowett on our article and what this might mean for the field moving forward…
Secondly, I wanted to share a poem about the relationship between gender and sex, I have written on these reflections in collaboration with ChatGPT. Please let me know your thoughts on these outputs in the comments.
In realms of knowledge, concepts intertwined, Where “gender” and “sex” are thoughts refined, “Sex” speaks of biology, physical and true, Reproductive traits and chromosomes in view.
But “gender” dances, a multifaceted tale, Constructed by society, a social trail, Roles, behaviors, identities enfold, In expectations and norms, stories unfold.
Male, female, intersex, the sex divide, But “gender” transcends, a fluid ride, A spectrum wide, beyond binary’s reach, Unveiling diverse expressions that beseech.
Yet understand, definitions sway, Disciplines and cultures, perspectives may, Vary in their interpretations and embrace, Of gender and sex, a scholarly space.
So, in the realm of knowledge’s delight, A simple “yes” or “no” won’t ignite, For complexity we seek to explore, In understanding gender’s dance, and more.
Until next time…Look after yourselves and each other
We recently had our research published in Gender & Society, and we wanted to thank all of you who gave your time to shape the direction of this research early on. We hope that further down you will help us shape the next phase too.. keep reading.
In line with the majority of contemporary Britons (Tryl et al. 2022), participants were highly trans and nonbinary positive. Participants were most confident in formulating care plans and least confident about the provision of colleagues’ perinatal care in this context. While the majority of participants were positive toward the trans and nonbinary communities, they considered that those communities remain marginalized in perinatal services. Transphobic, anti-trans, and nonbinary attitudes were highlighted by our respondents. Our findings suggest that caregivers witnessed transphobia among colleagues and were apprehensive themselves about providing care to childbearing trans and nonbinary people. They reported a cisheteronormative model of care that lacked awareness of trans and nonbinary issues. The educational needs identified included information about the practicalities of childbearing as a trans or nonbinary person, how to use inclusive language effectively, and creating policies and processes for supporting childbearing trans and nonbinary people. These caregivers’ preferences included hearing from trans and nonbinary people and sharing best practices among themselves, with open discussions about how to be inclusive.
Cisnormative, heteronormative, cisgender, and heteropatriarchal services, administrative procedures, structural forces, and interpersonal treatment combine in the perinatal space. In this study, we provide evidence that such institutionalized “support” is designed to reinforce a gendered experience of pregnancy and childbirth that marginalizes childbearing trans and nonbinary people who do not conform to cisgender ideals. This study also offers important insights as to how providers’ stances inform mundane cisgenderism, passive eugenics, stigma visibility, the minority stress model, and the “doing” and “undoing” of gender.
Health care providers may usefully reflect on whether their service provision could be more identity affirming for the trans and nonbinary communities they serve. Professional trans and nonbinary competent education is needed, and reproductive health services and systems must be more inclusive of trans bodies and identities. Thus, future professionals, systems, and services must be prepared for a new and more inclusive (rather than exclusive) reality.
Considering the findings presented above, please take a few moments to respond to our survey below… We would love to hear what you think!
Midwifery and ‘Maternity’ care has been theorised from feminist perspectives, as ‘woman centred’ care, focusing on women’s choice and autonomy in relation to how and where they give birth. Yet trans men and non-binary people are a growing population within ‘maternity’ services experiencing pregnancy, and birth. This poses challenges for midwives, as the retention of professional identity is considered to be the cornerstone of professionalism in healthcare.
Findings from our preliminary work in this area indicate that the strong identification of midwifery as a women’s profession being ‘with women’ also appeared in some cases to be a barrier to the inclusivity of service users who do not identify as women, leading to a range of adverse outcomes (e.g., service users forced to choose between embracing their core human rights to gender identity, and their sexual and reproductive health). Thus we have recently advertised a PhD studentship. The aims of which will be to:
Explore relationships between the midwifery profession and gender identity
Critically examine midwives’ everyday rhetorical discourse in relation to midwifing childbearing trans men and non-binary people
Develop an in depth understanding of midwives’ professional identity in the context of midwifing those who do not identify as women.
If you are interested in applying, please get in touch…
Until next time…Look after yourselves and each other
This month has been awards month. First of all I picked up the Partnership Working Award from the Royal College of Midwives on behalf of www.hEDSTogether.com…I was certainly not expecting this award given the fierce competition. I was also feeling terrible in recovery from a cold when I collected the award. So not the best look over all (red nose & tears!)
Next time I certainly need to dress up in something a little more sparkly….
It was awesome to spend the day among other ‘Tall Poppies’ celebrating… It has been such a long time since we have been able to meet as midwives in person! The Brewery was a wonderful venue and the organizing team had done a wonderful job! – Thank you!
Next we had the Student Nursing Times Awards… #STNA 10th Anniversary!
It is such a privilege to judge the category of the ‘Student Midwife of the Year’
Here I am bestowing the award upon the wonderful Nicolette Porter from Middlesex University!
Also wonderful to meet with other awesome academics at this event….so much to learn and share from the best in Higher Education. I am learning every day!
Until next time…Look after yourselves and each other
September 2021, we published the first research of it’s kind to explore problematic substance use in midwifery populations. The maternity and midwifery forum kindly shared our blog about this here.
You can read about our findings here or watch the video below for a short summary of what we found.
Main findings as follows:
• Just over ¼ of our sample (623 midwives) screened positive for problematic substance use (alcohol and a range of restricted drugs).
• Problematic substance use occurred reportedly in response to work-related stress and anxiety, bullying, traumatic clinical incidents and maintenance of overall functioning
• While 11% of those affected indicated they had sought help, 27% felt they should seek help but did not
• Barriers to help-seeking included fear of repercussions, shame, stigma, practicalities and a perceived lack of support either available or required
• 10% of the sample reported they had attended work under the influence of alcohol, and 6% under the influence of drugs other than tobacco or those as prescribed to them.
• 37% indicated concern about a colleague’s substance use.
Calling All Healthcare workers across the UK – The call-out for participants in this unique wellbeing project is now open with dates across 2021!
If you, or someone you know, would like to get involved – please follow the link to sign up: https://bit.ly/HNHform
The workshops aim to give space to participants, allowing for moments to decompress and process.
By taking part in this project, you will participate in co-creation workshops led by professional artists Caroline Horton or Rochi Rampal, you will collaborate with other healthcare workers from across the UK in a supportive online environment and co-create a unique piece of audio art work which represents your experiences of working through the pandemic.
There are four dates to choose from for Workshop 1. Workshop 2 is optional as the co-refinement process can take place via email. The sharing event is also optional and will be recorded for participants who are unable to attend.
All workshops will take place online.There are a number of dates available.
You can always see what studies we are recruiting for by clicking here.
As we come to the end of May 2021, I wanted to reflect on a few of the things which have come to fruition.
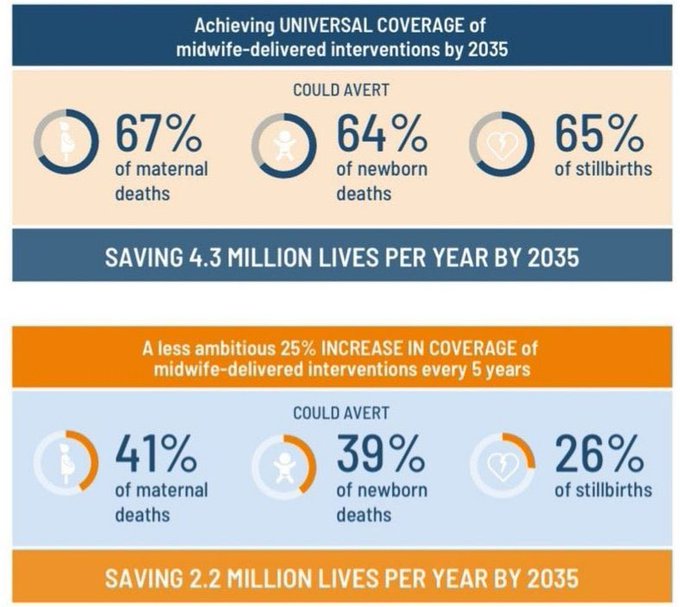
Of course early on we celebrated International Day of the Midwife 2021. Invest in midwives…The best is yet to come! #IDM2021
#IDM2021
On this #IDM2021 (May the 5th) I was thrilled to be able to announce some awesome things we have been working on for some time now. First, I was able to share our @IolantheMidwife ‘Midwives Award’ won on #InternationalDayoftheMidwife for our work on Substance use in Midwifery populations. You can still participate in this research until September 2021 – Details below. Please share this link with midwifery teams: https://bit.ly/UKMidwivesPSU
I was also able to share my appointment as #NursingNowChallenge midwifery champion!
I hope that this will be enable us to raise the profile of midwives around the world.
Furthermore, on the 6th May 2021 I had the privilege of being the invited speaker at the 102nd Irish Nurses & Midwives Organisation@INMO_IRL (@INMO_IRL) Annual Delegates Conference. #INMOADC. I shared our work ‘Exploring Problematic Substance Use in Nursing and Midwifery Populations’ – A warm audience as ever!
Thank you for having me.
#INMOADC
Then on the 18th of May 2021 I tuned in to watch the policy dialogue presenting the findings from #SoWMy2021 to Member States in an effort to encourage sustainable investment in the midwifery workforce. This was a really inspiring event where I was able to make some really valuable connections – thank you.
Other than May being my birthday month, May 2021 has been absolutely awesome. Moreover, I have been able to settle in in my new role as an RCM Fellow! Read more here
“Excited by what we may achieve together as this fellowship brings forward new opportunities…the best is certainly yet to come” says @SallyPezaro from @covcampus receiving RCM Fellowship#rcmedconf21 #education
Now that some of the restrictions are easing it seems that some publications are able to move forward again in the process of peer review. As such, I will be sharing some new publications with you all soon. I also have lots of bid writing plans for next month alongside teaching. A summer of collaborations ahead.
First, I am grateful for the opportunity to continue and finish journey with @OxfordSBS … because midwifery #LeadershipMatters
Until next time…Look after yourselves and each other
Applications for babies to be taken in to care at birth are at a national high. This results in significantly impaired life outcomes for the birthing community and their babies. So what barriers and facilitators are at play here? We have produced the following review of the literature published in @BJMidwifery to uncover therapeutic mechanisms and interventions to support those at risk of having their baby removed from them at birth.
The development of strong professional relationships
Early and sustained interventions
Uniquely, using the themes presented within this review, we have been
able to model the cycle of maltreatment which needs to be broken in Figure 1.
As this review only yielded eight studies in total, further research could usefully inform a richer provision of research inspired teaching and training in this area.
For some years now I have had the pleasure of marking student essays and reading their interesting ideas and arguments in relation to a number of healthcare topics. Yet repeatedly, I see the same mistakes being made. These mistakes mean that I cannot assign a higher mark to the work, and that makes me sad. So, I’ve tried to consolidate and explain how to avoid the top 10 essay mistakes.
Want to know how to get higher marks in your essay? Read on…
Top 10 Mistakes Students Make in Their Essays…
Always explain acronyms the first time you use them
Many students simply start using acronyms without explaining what they mean. How to fix this? You explain and write first that you are speaking in relation to the United Kingdom (UK)….THEN you can use ‘UK’ throughout the rest of the essay. If you don’t explain it first then I am left guessing as to what you mean throughout the rest of the work.
This word is often spelled incorrectly. How do you know when to add an ‘S’ or a ‘C’? Try replacing the same sentence with the word ADVICE or ADVISE. The one which sounds more appropriate tells you which to use. For example:
Fitness to ‘advise’ sounds more appropriate than Fitness to ‘advice’. Therefore in this sentence you would spell practice with an ‘S’ so… the correct spelling in this case would be…
Fitness to PractiSe
3. avoid getting your essay structure back to front
Sometimes things can get higgledy piggledy. Your work should flow logically like a story, and it’s structure will depend largely on your own assignment guide….but broadly, appendices will go after reference lists and be labelled and named. You will also need to mention appendices, tables and figures in the main body of the text in order to direct the reader as to where to find things.
A story – a beginning, a middle and an end. Try to follow a narrative structure and your discussions and arguments will follow suit…the best way to do this is with structured assignment planning; each concept and new idea should link together or follow a new introduction.
One single sentence alone does not make a paragraph, yet too often I see this in essays, and it is not particularly useful. Also, I have yet to see anyone make a strong and well reasoned and evidence based argument in only one sentence. More often than not, this will be a single statement, best avoided unless coupled with other meaningful text.
5. Avoid huge chunks of text
A large chunk of text will likely have several points and arguments within it which can get lost overall. If you can break up such large chunks of text into smaller paragraphs, your overall structure will be far stronger. Each paragraph should encompass one argument concisely.
When an essay gets a low grade, it is often because the reader is unconvinced of the arguments being made. Sometimes arguments do not go far enough, they are often not concluded. Ensure that you conclude each argument, after you have cited the evidence which lays out your case. For example, you may start the paragraph by saying….
“Johns et al (2020) explain how you can scald yourself by not wearing oven gloves when baking. Equally, Kent et al (2020) emphasize the need to wear oven gloves in the context of cooking in the kitchen. Nevertheless, another study proved that simply letting the oven dish cool down is effective enough in preventing burns in this context (Frog et al, 2020).”
The above example is similar to what I see in a lot of essays. Yet in itself, it does not round up an argument or make a case. It simply states what the evidence is in relation to the topic. To complete the argument, the author needs to draw a conclusion on this. What does this mean? what implications does it have? How strong or weak is the evidence in this regard. This paragraph does not go far enough, and ultimately needs concluding with another sentence or two beginning (for example) with… Therefore… or…As such…(insert very insightful conclusion here).
7.AVOID MAKING LARGE STATEMENTS WITHOUT BACKING THEM UP
Unless you are a world leader or significant and respected public figure, I am afraid you must avoid making large sweeping statements in a sentence without citation. For example, poverty may be a well known issue in many parts of the world. Yet you cannot simply say this (obvious though it may be) without citing a reference which points to the evidence for it. I frequently see this occurring in student essays – I can never assign positive marks to this.
8.ENSURE YOU ARE USING APPROPRIATE REFERENCES
The appropriate use of citations and references is a good thing. It demonstrates evidence of wider reading and makes your arguments stronger. However, the references used must be appropriate in the context of your work and field. In academia, it is generally most appropriate to cite peer reviewed articles from academic journals. Magazines and newspapers may be appropriate to cite in some cases, especially in some specialist fields. However, in nursing and midwifery for example, articles from publications such as ‘The Nursing Times’ will often be secondary sources reporting on the evidence, rather than the primary source of evidence itself. It is always best to cite the primary source of evidence in such cases.
In terms of referencing style, it is important to get this right too. See your own institutions style guide for the particulars.
Top Tip: Google Scholar will give you the top referencing style formats by clicking on the ‘cite’ button under each item listed. Click the ‘ “ ‘ symbol.
Too often I see students relying too heavily on the work of others. You should only be referring to the work of others in order to strengthen your own insights and arguments. I cannot give you marks for only telling me what other people say.
10.AVOID BEING OVERLY DESCRIPTIVE
All too often, I see entire paragraphs describing what happened in a particular research study. I can give no marks for this as it is ultimately description. Moreover, I can read the study for myself, so you only really need to give a small description of the study to set the context for what you are trying to say. For example, if you want to talk about the rigor of a study design, all I really need to know is the study design in question. The marks come where you critique, rather than simply describe.
A useful paragraph may begin…
The study by Arthur et al, (2020) included a randomized controlled trial (RCT). RCT’s are generally considered rigorous when….(insightful critique continues)…