Whilst I am sure that there are many reputable companies who will publish your thesis out there, I wanted to share with you all how I published mine.

First of all, I believe that if you have a PhD then your work must be adding some original knowledge to the world. That means that your work is of value, and should therefore be published and disseminated widely. This is also true for students, whose work is of great value to the academic community.
But here, I wanted to map out one way to publish your thesis. It is the way I published mine.
Step one…
Publish background literature reviews to outline how you arrived at your research questions. Much of this work will summarize the first chapters of your thesis. It will also help you refine your ideas if you publish as you write.
My initial chapters were published as follows:
Pezaro, S The midwifery workforce: A global picture of psychological distress – Article in Midwives: Official journal of the Royal College of Midwives (2016): 19:33
Pezaro S Addressing psychological distress in midwives. Nursing Times (2016): 112: 8, 22-23.
Pezaro, S., Clyne, W., Turner, A., Fulton, E. A., & Gerada, C. (2015). ‘Midwives overboard! ‘Inside their hearts are breaking, their makeup may be flaking but their smile still stays on. Women and Birth 29.3 (2016): e59-e66.
Step two…
Publish your ideas around the theories used in your work.
I did this by publishing a blog on theories of work-related stress. I also published a paper exploring the ethical considerations of what I was trying to do entitled ‘Confidentiality, anonymity and amnesty for midwives in distress seeking online support – Ethical?’. Opening this up for discussion meant that my thesis was much stronger overall.
Step three…
Publish your methods via research protocols.
Not only does this mean that you have claimed the idea for yourself in the academic world, but you also then get the benefit of a wider peer review of your work. I published the protocol of my Delphi study as follows:
Pezaro, S, Clyne, W (2015) Achieving Consensus in the Development of an Online Intervention Designed to Effectively Support Midwives in Work-Related Psychological Distress: Protocol for a Delphi Study. JMIR Res Protoc 2015 (Sep 04); 4(3):e107
Step four…
Publish each chapter of your work as you go.
Again, this gives your work added peer review in the process of developing your thesis. I published the two largest pieces of research in my thesis as follows:
Pezaro, S, Clyne, W and Fulton, E.A “A systematic mixed-methods review of interventions, outcomes and experiences for midwives and student midwives in work-related psychological distress.” Midwifery (2017). DOI: http://dx.doi.org/10.1016/j.midw.2017.04.003
Pezaro, S and Clyne, W “Achieving Consensus for the Design and Delivery of an Online Intervention to Support Midwives in Work-Related Psychological Distress: Results From a Delphi Study.” JMIR Mental Health3.3 (2016).
Step five…
Publish summaries of your work for different audiences
Once you begin to pull together your entire thesis, you will begin to discuss the findings and arrive at certain conclusions. You can summarise these in a series of blogs and papers as you go. I published the following summary papers to reach both national and international audiences.
Pezaro, S (2018) Securing The Evidence And Theory-Based Design Of An Online Intervention Designed To Support Midwives In Work-Related Psychological Distress (Special Theme on Women in eHealth). Journal of the International Society for Telemedicine and eHealth. Vol 6, e8. 1-12.
Pezaro, S “The case for developing an online intervention to support midwives in work-related psychological distress.” British Journal of Midwifery 24.11 (2016): 799-805.
Step six…
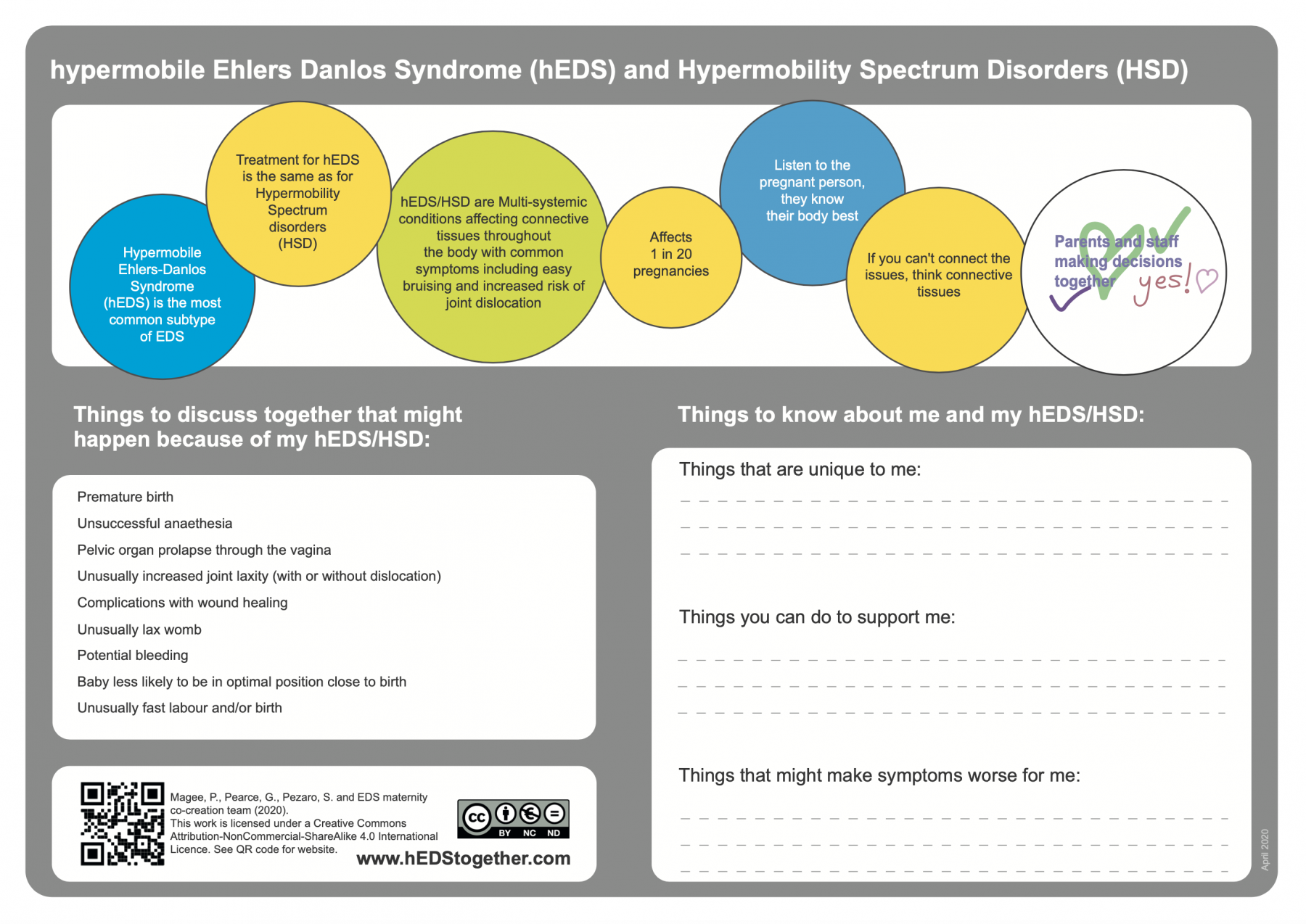
Use info graphics to map out key points in your thesis
Once complete, your thesis will be published in full. Mine can be accessed here via the British Library and via Coventry University’s open collections. But it’s a mighty big document. Therefore, I produced the following infographic to map out my PhD journey for those looking for a shorter, yet engaging summary.

…and there you have it. A fully published PhD thesis via a variety of avenues. I hope that you enjoy publishing your PhD thesis, and that publishing it helps you to defend it.
Also…If you need a co-author, let me know!🎓😉
If you would like to follow the progress of my work going forward..
Follow me via ; The Academic Midwife; This blog
Until next time…Look after yourselves and each other 💚💙💜❤