This is the research blog of Dr Sally Pezaro. Dr Pezaro is working to secure excellence in perinatal services. Specialist interests include workforce, gender and midwifery research.
I would love to hear your ‘respectful’ thoughts and views here. I have to admit I watched in through my fingertips and found it quite triggering. This issue I have is that I would love to see the real lives of healthcare professionals portrayed through drama. Nevertheless, it is not a comedy out there.
I heard one interesting view from a woman who had experienced a traumatic birth. She found it cathartic and helpful to think of staff as being human in this way. What are your thoughts?
Until next time…Look after yourselves and each other
I was privileged to be asked to perform and write up the analysis for this report. The findings truly moved me. If you know my work at all, you will know that it is heavily focused upon securing the psychological wellbeing of midwives. This is because I do not believe that excellence in maternity care can be delivered to mothers and babies without the provision of effective support for midwives.
Findings here revealed that some midwives trained to recognise domestic abuse and support women, were sometimes not recognising that they themselves are victims of domestic abuse.
“I was allowed to stay overnight on my delivery suite to avoid going home to my abusive partner”
“I was made to feel I was a nuisance, constantly asking me and contacting me, pressurizing me in to coming back to work. I gave in and did but I was soon off again as I still wasn’t well, and I then left midwifery because I didn’t want to be dismissed. I didn’t receive any support that was effective for me”
“I have and was been treated very badly by my place of work, absolutely no support or care and compassion”
“I was given a specific senior midwife who I could go to for support, to discuss things at times when home was particularly bad and to deal with any sickness absence – helpful as one person knew what was going on and I could be truthful, especially about the reasons for sickness absence sometimes”
“All staff should be asked about domestic abuse or violence on a regular basis”
“Police and social services were unhelpful, and no support provided. Neither I nor my children were offered counselling or directed to appropriate services despite asking several times for help. One police officer even commented that due to my ethnicity I could handle the situation myself.”
Based on the findings the RCM has put forward the following evidence-based recommendations. These will enable maternity service managers and NHS Trusts/Boards to support staff experiencing domestic abuse more effectively.
All NHS Trusts/Health Boards should develop specific policies to support who are victims of domestic abuse, aligned to existing guidance from the NHS Staff Council developed in 2017.
NHS Trusts/Health Boards should provide and publicise confidential domestic abuse support services for affected staff, including access to IDVAs, external counselling and legal services as appropriate.
NHS Trusts/Health Boards should ensure that all managers and supervisors are trained on domestic abuse issues, so that they can recognise signs of domestic abuse in their staff and confidently undertake their safeguarding obligations.
NHS Trusts/Health Boards should ensure that staff at all levels are trained on domestic abuse issues and made aware of relevant workplace policies as part of their induction programme and continuous updating and are made aware of support services.
It was a pleasure to work with esteemed colleagues at the RCM to put this report together. Midwives and maternity support workers are a highly valued workforce whom we rely on to provide optimal care for mothers and babies. It is our sincere hope that this report will enable maternity service managers and NHS Trusts/Boards to support staff experiencing domestic abuse more effectively.
“Thank you to all of the midwives and maternity support workers who took part in this survey. The wellbeing of maternity staff is intrinsically linked with the safety and quality of maternity services. Your thoughts, feelings and experiences have helped us to arrive at a deeper understanding of the resources required to support those experiencing domestic abuse.”
If you would like to follow the progress of work going forward..
We are all well aware of how the wellbeing of healthcare staff can affect the quality and safety of care. I have also talked at length about the wellbeing of health care staff and the theories surrounding work-related psychological distress. But do we really have any concrete idea of what shows workplace compassion for healthcare staff?
My research published in collaboration with Dr. Wendy Clyne, Dr. Karen Deeny and Dr. Rosie Kneafsey asked Twitter users to contribute their views about what activities, actions, policies, philosophies or approaches demonstrate workplace compassion in healthcare using the hashtag #ShowsWorkplaceCompassion. It can be cited as follows:
Recently, the wonderful Ibone Olza (Perinatal Psychiatrist and Childbirth Activist from Childbirth is Ours, Spain) contacted me about her work on obstetric violence, birth rape and professional trauma. After reading her papers and watching her present her work, I was compelled to document and reflect upon some of the issues raised, here.
The following points are made within the paper: Fernández, Ibone Olza. “PTSD and obstetric violence.” Midwifery today with international midwife 105 (2013): 48-9.
Birth trauma has been defined as “Actual or threatened injury or death to the mother or her baby” (Beck 2008). Yet such trauma lies in the eye of the beholder, therefore, any trauma experienced by either the mother, newborn or the birth attendant may be due to a subjective experience of stress which does not need to fit any particular criteria necessarily. This means that some traumatic events may be subjective in their nature, and as such, we cannot judge what may or may not cause another person trauma. It is a personal interpretation or perception.
A meta-ethnographic analysis of studies about women’s perceptions and experiences of a traumatic birth reported that women are often traumatized as a result of the actions or inactions of midwifery staff (Elmir et al. 2010). Whatever, such inactions or actions may be…women often use words such as ‘barbaric’, ‘intrusive’, ‘horrific’ and ‘degrading’ to describe their mistreatment (Thomson and Downe 2008).
For Hodges, drugging or cutting a pregnant woman with no medical indication is an act of violence, even when performed by a medical professional in a hospital. Inappropriate medical treatment is also clearly abusive, although few women are aware that this is deliberate mistreatment (Hodges 2009).
The term ‘birth rape’ has been used by women who feel that their bodies have been violated. Kitzinger highlighted that many women who have experienced a traumatic birth display similar symptoms to rape survivors (Kitzinger 2006). The video below explores these issues in greater detail, as we can hear the lovely Ibone Olza sharing this work.
One of the things I was most encouraged about, was that Ibone Olza considers the wellbeing of the midwifery staff in her work. Birth attendants are often also traumatized by these acts, and may feel powerless to intervene. In a recent study by Beck, 26% of obstetric nurses met all the diagnostic criteria for screening positive for PTSD due to exposure to their patients who were traumatized (Beck and Gable 2012). Being present at abusive deliveries can magnify staffs’ exposure to birth trauma.
staff use phrases such as…
“the physician violated her”
“a perfect delivery turned violent”
“unnecessary roughness with her perineum”
“felt like an accomplice to a crime”
“I felt like I was watching a rape.”
….to describe the guilt that ensued when they felt like they had failed women or they did not speak up and challenge/question…
Article 51 establishes that: The following acts implemented by health personnel are considered acts of obstetric violence:
Untimely and ineffective attention of obstetric emergencies
Forcing the woman to give birth in a supine position, with legs raised, when the necessary means to perform a vertical delivery are available
Impeding the early attachment of the child with his/her mother without a medical cause thus preventing the early attachment and blocking the possibility of holding, nursing or breastfeeding immediately after birth
Altering the natural process of low-risk delivery by using acceleration
techniques, without obtaining voluntary, expressed and informed consent of the woman
Performing delivery via cesarean section, when natural childbirth is possible, without obtaining voluntary, expressed, and informed consent from the woman
(D’Gregorio 2010)
Yet whilst people do bad things, it is important to remember that they are not necessarily bad people…
This work explains how professionals may exert obstetric violence due to:
Lack of technical skills to deal with emotional and sexual aspects of childbirth.
Unsolved trauma. The medicalization of childbirth produces more severe iatrogenic
complications (Johanson, Newburn and Macfarlane 2002; Belghiti et al. 2011). If the
professionals do not have a supportive space to reflect or to deal with this aspect of iatrogenic care, they may fall into a spiral of continuously increased medicalization as a defensive strategy. Childbirth is then perceived as a very dangerous event, “a bomb ready to explode,” without realizing that interventions cause more unnecessary interventions and pain.
Professional burnout in birth attendants will lead to increased dehumanized care and therefore never-ending figures of women experiencing childbirth as very traumatic.
..and so the challenge will be to identify and address these root causes to ensure that maternity staff are able to provide excellence in midwifery care. My work explores how we might support the psychological wellbeing of health care staff may increase levels of humanity and compassion in care. I hope to keep in touch with Ibone Olza and many others around the world who share the same passion for this work. Together we may collectively work towards a time where maternity workers are psychologically safer, and therefore better able to provide the excellence in care they strive to give.
If you would like to follow the progress of my work going forward..
Until next time…Look after yourselves and each other 💚💙💜❤
References and further reading
Soet JE, Brack GA, DiIorio C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth 2003 Mar;30(1):36-46.
Creedy DK, Shochet IM, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000 Jun;27(2):104-111.
Ayers S, Pickering AD. Do women get post traumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001 Jun;28(2):111-118.
Beck CT, Gable RK, Sakala C, Declercq ER. Post traumatic stress disorder in new mothers: results from a two stage U.S. national survey. Birth 2011 Sep;38(3):216-227.
Allen S. A qualitative analysis of the process, mediating variables and impact of traumatic childbirth. Journal of Reproductive and Infant Psychology 1998;16(2-3):107-131.
Beck CT, Watson S. Impact of birth trauma on breast-feeding: a tale of two pathways. Nurs Res 2008 Jul-Aug;57(4):228-236.
Beck CT. Post-traumatic stress disorder due to childbirth: the aftermath. Nurs Res 2004 Jul-Aug;53(4):216-224.
Beck CT. Birth trauma: in the eye of the beholder. Nurs Res 2004 Jan-Feb;53(1):28-35.
Ayers S. Delivery as a traumatic event: prevalence, risk factors, and treatment for postnatal posttraumatic stress disorder. Clin Obstet Gynecol 2004 Sep;47(3):552-567.
Olde E, van der Hart O, Kleber R, van Son M. Posttraumatic stress following childbirth: a review. Clin Psychol Rev 2006 Jan;26(1):1-16.
Elmir R, Schmied V, Wilkes L, Jackson D. Women’s perceptions and experiences of a traumatic birth: a meta-ethnography. J Adv Nurs 2010 Oct;66(10):2142-2153.
Nicholls K, Ayers S. Childbirth-related post-traumatic stress disorder in couples: a qualitative study. Br J Health Psychol 2007 Nov;12(Pt 4):491-509.
Ayers S. Thoughts and emotions during traumatic birth: a qualitative study. Birth 2007 Sep;34(3):253-263.
Thomson G, Downe S. Widening the trauma discourse: the link between childbirth and experiences of abuse. J Psychosom Obstet Gynaecol 2008 Dec;29(4):268-273.
Goldbort JG. Women’s lived experience of their unexpected birthing process. MCN Am J Matern Child Nurs 2009 Jan-Feb;34(1):57-62.
Sawyer A, Ayers S. Post-traumatic growth in women after childbirth. Psychol Health 2009 Apr;24(4):457-471.
Hodges S. Abuse in hospital-based birth settings? J Perinat Educ 2009 Fall;18(4):8-11.
Kitzinger S. Birth as rape: There must be an end to ‘just in case’ obstetrics. British Journal of Midwifery 2006;14(9):544-545.
Beck CT. The anniversary of birth trauma: failure to rescue. Nurs Res 2006 Nov-Dec;55(6):381-390.
Beck CT, Gable RK. A Mixed Methods Study of Secondary Traumatic Stress in Labor and Delivery Nurses. J Obstet Gynecol Neonatal Nurs 2012 Jul 12.
Perez D’Gregorio R. Obstetric violence: a new legal term introduced in Venezuela. Int J Gynaecol Obstet 2010 Dec;111(3):201-202.
Johanson R, Newburn M, Macfarlane A. Has the medicalisation of childbirth gone too far? BMJ 2002 Apr 13;324(7342):892-895.
Belghiti J, Kayem G, Dupont C, Rudigoz RC, Bouvier-Colle MH, Deneux-Tharaux C. Oxytocin during labour and risk of severe postpartum haemorrhage: a population-based, cohort-nested case-control study. BMJ Open 2011 Dec 21;1(2):e000514.
Reducing stress and fatigue among maternity staff is key to reducing baby deaths and brain injuries during childbirth, according to a detailed new analysis published by the Royal College of Obstetricians and Gynecologists.
This ‘each baby counts’ initiative confirms that “Decision-making is more difficult when staff feel stressed or tired”.
“This report shows that there is a need for additional support for our maternity staff and units so that every mother and every family has the healthiest possible outcome from pregnancy and birth,” said Judy Ledger, founder and chief executive of the charity Baby LifeLine.
This news supports my own research quest, as I work to find new interventions to support midwives in work-related psychological distress.
This state of affairs also suggests that it may be prudent to do all that we can to ensure midwife satisfaction in the workplace. In fact, anything good in the workplace has to be safer/better than the bad stuff right?
At the 31st International Confederation of Midwives’ Triennial Congress held in June 2017, I stumbled upon an interesting research presentation on what could promote satisfaction/dissatisfaction in the midwifery workplace. More specifically, the characteristics of midwifery management behaviors were used to demonstrate what might promote satisfaction and dissatisfaction in managerial relationships. I will translate my brief notes from the session here:
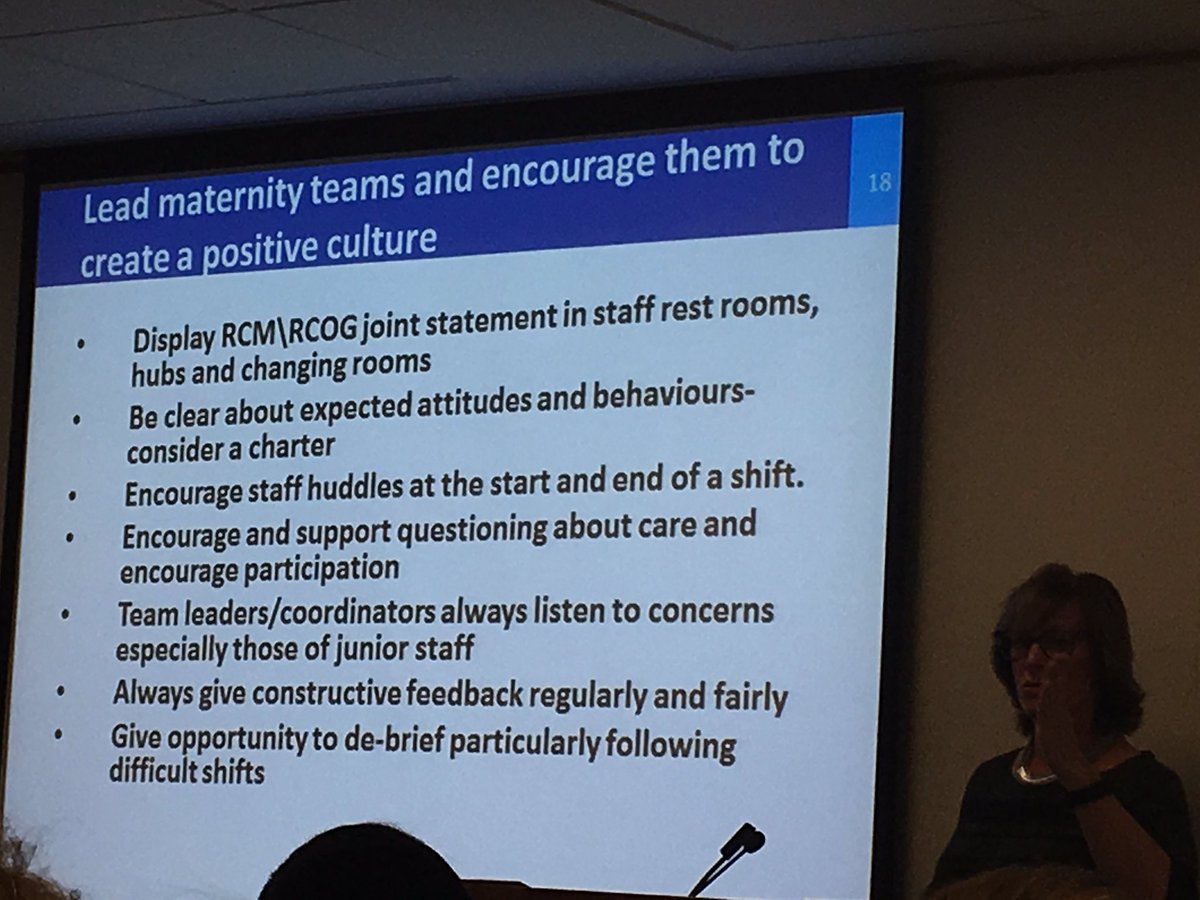
In promoting workplace satisfaction, a midwifery manager:
Is supportive
Respects, values and appreciates midwives
Is an advocate for staff
Follows through on promises
Facilitates new ventures and learning
Cares for staff
Is aware of stressors
In promoting workplace dissatisfaction, a midwifery manager:
Is punitive
Is demanding
Is inconsistent
Is ineffectual
Is ‘Terrible’
Tolerates or perpetrates bullying
Does not listen
Not a big shock here right?…I mean it’s not rocket science. Nevertheless, this knowledge must be shared in order to promote healthy workplace cultures in the pursuit of excellence in maternity care.
The best midwifery care can only be delivered by midwives at their best…. Can we all begin to set our working day by these rules? Can we all be a little kinder? caring?..respectful to one another?
This was just one of the many things learnt at this year’s #ICM2017#ICMLive.
Happy #internationaldayofthemidwife or (#IDM2017) as it is indeed the 5th of May 2017. I wanted to do a quick reflection (and a little dance of happiness) about the fact that the focus of this year’s International Day of the Midwife is…
“Midwives, Mothers and Families: Partners for Life!”
With messages coming from the International Confederation such as…”It is very important that midwives and mothers both acknowledge the reciprocity of their relationship” – Scarlett #IDM2017@ToyinSaraki
Yes…..we work in PARTNERSHIP with women and their families!…mothers, families and midwives are all equal partners….this means that we can finally break the mold and state openly that we, as midwives can also be prioritised!…Fabulous!
I have often wondered whether terms such as ‘Patient comes first’ is really healthy…as it is terms like this which often infer that midwives come second at best. What do you think?
I have also been picking up on some other great messages, pictures and videos this #IDM2017..such as…..
— Rachel Ellie Gardner (@RachelEllieG) May 5, 2017
I have also been dipping in and out of the Virtual International Day of the Midwife conference sessions a FREE conference that happens online every year….I have presented my work at @VIDofM (#vidm17) before, and it is such a great opportunity to get people together in one place from all over the world!
This year for #Internationaldayofthemidwife I have recorded a podcast ‘Made by midwives for midwives’. Hosted by London based midwives Anthonissa Moger and Kate Whatmough…. (The Midwifery Podcast: Os closed, go home.)..I will be sharing this in an upcoming blog post…but for now..I am off to enjoy the rest of #IDM2017…there is such positivity in the midwifery world today…Let’s keep the momentum going ❣🎓❣
If you would like to follow the progress of my work going forward..
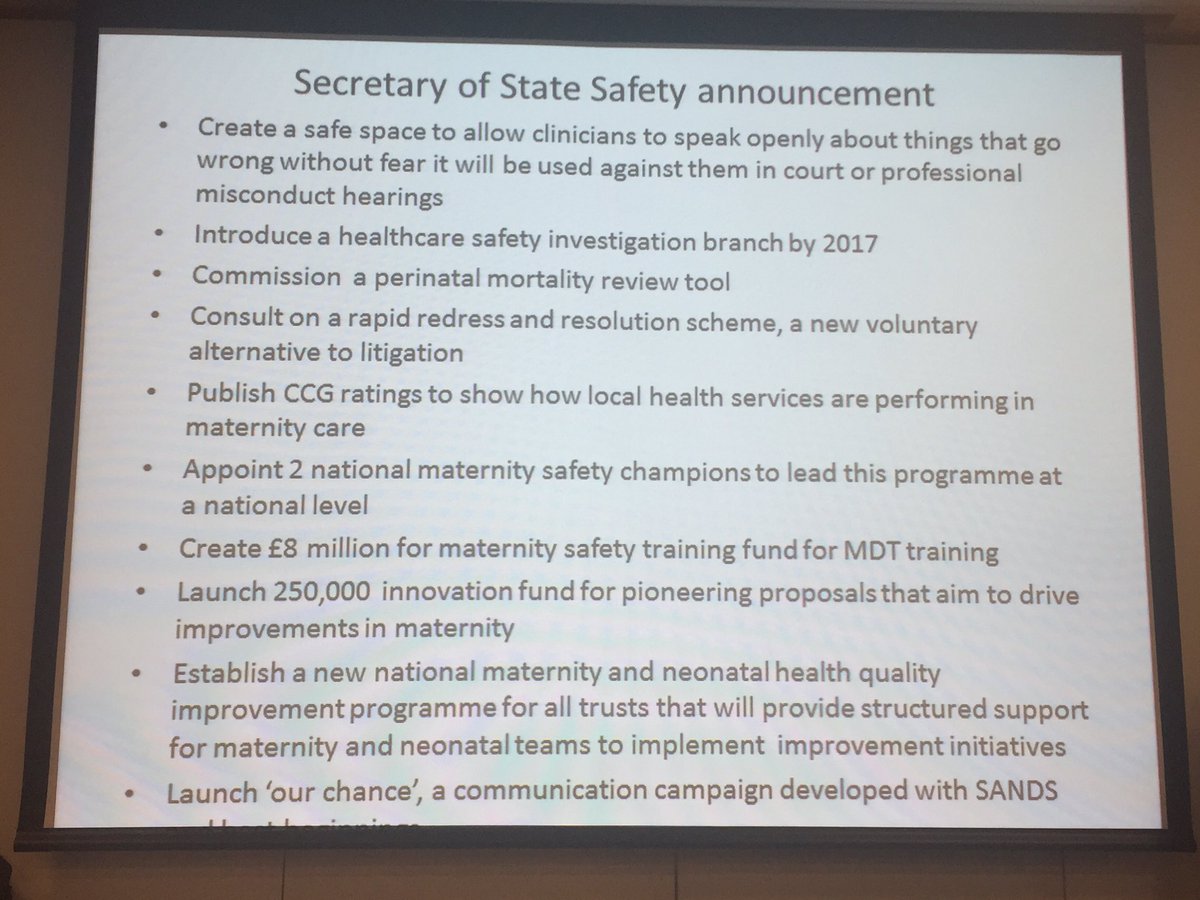
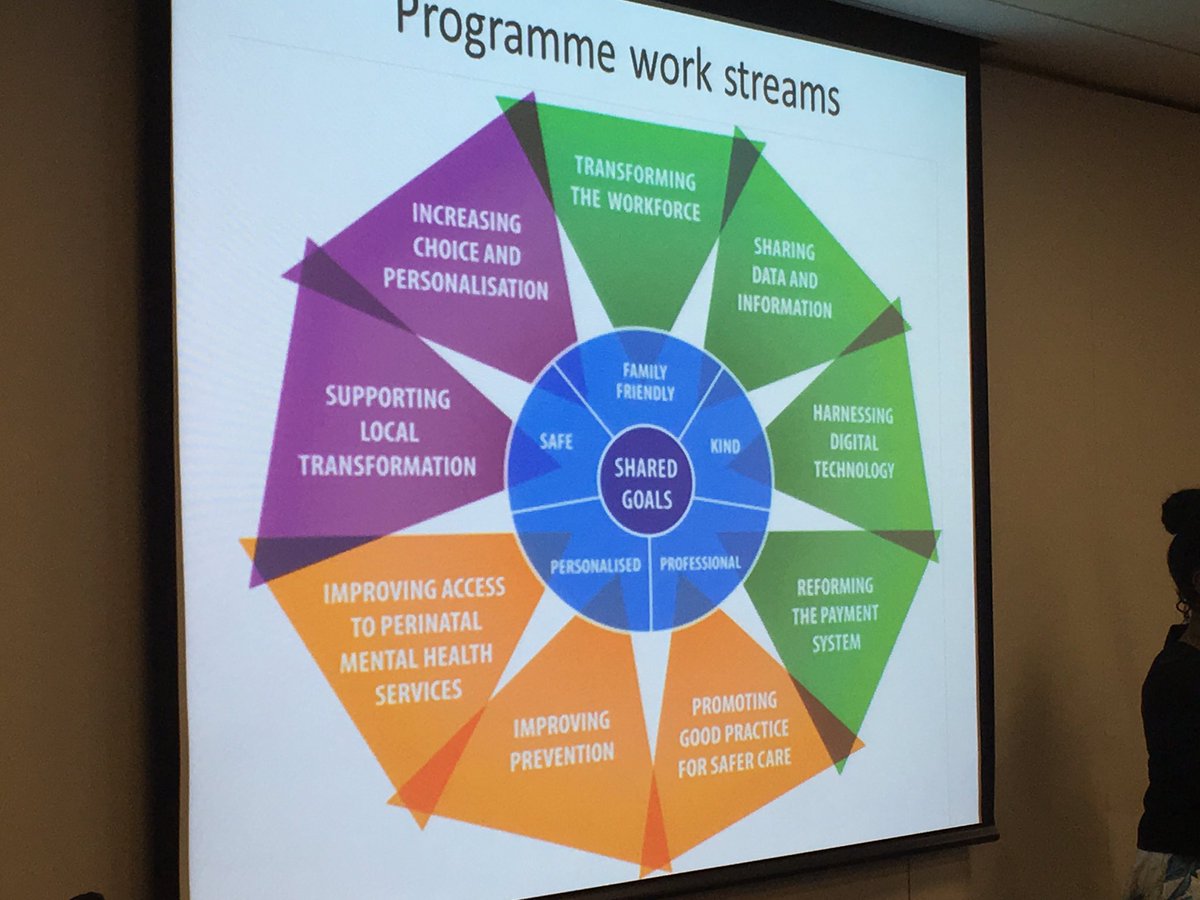
Attending and presenting work on midwife wellbeing at #uclhmw2016, I was thrilled to see so much of one conference dedicated to supporting the midwife, as well as the mother. I was also keen to hear Jacqui Dunkley-Bent update us all on the new plans for maternity services in 2017! – Bring it on!
-Improvement in Perinatal mental health in maternity services was highest on the agenda as we can see here – midwives were really responsive to making these a commitments a reality.
Yet we can see that NHS England is also looking to transform the workforce as part of this plan. There are so many ideas buzzing around my head at the moment that I am feeling dizzy… “so much to do and so little time” – As Willy Wonka would say.
We also saw how mothers are experiencing poor support in decision making…
There are so many great resources available from dignity in childbirth @birthrightsorg… We really need to challenge the way that women experience respect in maternity care.
Sadly, bullying still a real issue in midwifery, as @JacqueGRCM confirmed … punity, public shaming & undermining must stop.. We must be kinder to one another…remember why we became midwives in the first place and love each other for the critical safety of mothers and their babies.
There is indeed much to be done. I wanted to personally thank @Yanarichens, and @MaureenMcCabe15 (and their teams) for looking after me so well as a speaker at this conference myself. I have never been so well looked after at a conference 😘😍
And thank you to all of those who appreciated my presentation and engaged in this very important work. I love this particular image that people have been sending me (see below)…I believe it was created at the#BirthTrauma2016 conference & shares a powerful message 💜💙❤💚
There really is so much to do and so little time!
As a last thought introduced to us by Sheena Byrom ‘Midwives are humming birds never too small to make a difference’
Until next time – Take care of yourselves & each other ❤💚💙💛
An academic career has been described as a journey filled with brutal, unrelenting rejection. I frequently find myself having to pick myself up from rejection. It is hard.
Whether it is a paper in a journal, a grant application, your viva or an idea that you have lovingly nurtured and come to love and cherish, there are 5 stages of rejection grief that are more or less inevitable (for me anyway).
Having your work rejected can feel like you have just spent a lifetime nurturing and rearing a beloved child, only to find out that it has grown into an evil and murderous human being in need of ‘Major revisions’!
1. Denial and isolation
This is wrong. It cannot be. I was so certain that my work was beautiful!…I don’t want to talk about it 😦
2. Anger
How dare the reviewer pull apart my work in this way…do they know nothing???!!
3. Bargaining
OK, I will take a look at the revisions. I will accept comment 4 and 5, but I’m not doing what reviewer 3 wants!
4. Depression
Gah!….these revisions are so laborious and depressing.
5. Acceptance
Oh…OK…phew… it is done. I am happy with it. I am at peace and ready to resubmit!
Feedback is golden…but it can be challenging to accept…it feels like rejection….but we are all actually moving forward ..all of the time. See here about the importance of feedback. I don’t believe that managers, reviewers or examiners are out to get us (not all of them anyway)….and so we must remember that none of this is personal. It is not a rejection of you as an entity, it is a very subjective point of view which may actually improve the work you do.
Try to portray humility and gratitude…Rather than any knee jerk feelings…
“I’m sorry… you’ve got major revisions to do”
Work that needs major revisions? How will people judge that? How will I be judged? is everything I thought I knew a lie?..what would another reviewer have said? (Most of the time the reviewers all want different things in any case)!
Self doubt, career doubt, black and white thinking and a feeling of doom sets in. ‘I am not good enough’…I begin to catastrophise. But then I reflect…what is really behind success?
I think that my approach to revisions needs major revisions. I continue to work on these revisions daily….
Every piece of work that I have ever revised following feedback or rejection has improved. Yet every time…I have to put all of my toys back into my pram before I begin the process of making any changes. I go back and forward around the 5 stages of academic grief..round and around…but it always ends up fine in the end….mostly it ends up better.
I live in constant fear of rejection, failure and disappointing those who I respect most… But we must try to get over our fear of failure and rejection, or we loose the opportunities we have to learn and grow.
Remember…things always feel better in the morning…you will not always feel this way. The cure for academic rejection grief is not always instant success…it is compassion for both yourself and others.
Until next time, take care of yourselves and eachother ⭐🎓⭐
Recently, I was asked by Dr. Gloria Esegbona from the @art_of_birth to share some of my thoughts on birth trauma at the latest #artofbirth16 summit at Kings College London. My first thought, as always was…. do you mean physical? or psychological?… I was assured that her latest event would be addressing both. Time to learn & grow 💚💜❤
And so how can we as midwives prevent physical birth trauma?
I was quoted on this day when talking about “superhero midwives” – healthy, well-supported #midwives lead to healthy, well-supported mums. #artofbirth16…It is true…so many people wanting to do good….some burning out. Some traumatised.
I had some really great panel questions too…What I loved most about this conference was that I managed to receive lots of #Oxyhugs and create #myomos with so many inspiring midwives, doulas, students and others wanting to support each other, share and learn 💚💜❤.. I can’t wait to see some of you in the near future and learn more about how you have turned these lessons into practice. 💚💜❤
Until next time – look after yourselves and each other #GetYourGeekOn 💚💜❤
Another guilt trip about the importance of self care and being successful? That is why many people will read blog posts like this. We know we should be practising self care and succeeding, but do we really know how to thrive?
(I could not find a concept analysis for either success or self care – please let me know if you do)
We must presume that both success and self-care mean something different to each and every one of us. I am no expert on these topics…. is anyone?…But I think I am pretty good at caring for myself now and working towards success…having learnt the hard way. So I thought I would share some of my hints and tips. Feel free to adapt them, use them, completely ignore them, or ridicule them as ‘poppycock’.
Most people will expect to hear things like:
Take a bubble bath
Watch your favorite film
Curl up with a good book
Work hard
Network
But I am sure that you know about this kind of stuff already. So let’s look at self care and success for the academic, firstly by identifying the issues that some of us may face.
Tip One: Keep your eye on the goal. Visualize yourself being happy, frequently. How would it feel to publish that paper? Get that fellowship? Collaborate on that project? Create your own self-fulfilling prophecy rather than focus on a possible spiral of doom.
How to do this? – Identify what makes you happy, or what will make you happy. Then do more of what makes you happy, or have a real go at getting what will make you happy. I personally love my research work. I know that many other academics feel the same way. Happiness to me is succeeding, making a difference and making a real impact through my work. The stress I feel is associated with this not happening.
This stress and negative thinking serves no purpose unless it positively drives me towards my goal. Yet who wants to be whipped to the goal posts? I use visualization as a driver for success. I see myself feeling and being the way I want to be…and I allow myself to believe that this vision will come true. This makes me much happier than thinking about the alternative. So I stick with it.
The practice of meditation may also assist you to work through your thoughts, direct them towards a more positive outlook and allow your goals to become meaningful and achievable.
As these tips continue, think about your own goals for happiness…whatever they may be…think about achieving them in relation to these tips and your own experiences.
I behave in the way I want to feel or be… Surely if I continue in this direction. Good things will come…
Tip Two: The problem of job insecurity for early career academics baffles me as Job security for early career researchers is a significant factor in helping research make an impact. Yet this seems to play on my mind recurrently. It is always a worry. However, worry really does nothing to resolve this issue, and only seeks to get in the way of my progress. In order to progress, I will need to ‘work smarter’ and embrace confidence in my own abilities. Worry and negative thinking has no place in this strategy.
Negative thoughts often lie, and so I swipe them away one by one by placing them on a train that is passing the station (Visualization) – I then sit for a little longer, and imagine the way I will feel and be once I reach my goals. My mood and stress instantly lifts once I do this. I am more confident and feel much stronger. I am ready to be happy.
Tip 3: Say No and be proactive – We need to look at what successful academics do. From my observations, they often say ‘No’ to anything that doesn’t suit their own focused agenda (they remove the ‘noise’ and toxicity), they ooze positivity, they are confident, they are assertive, they tell people what they need to succeed and they hang around with the most inspiring people. Therefore, the most obvious strategy is for us to do the same. Say ‘No’ to negativity, and to the people and things which do not enrich us as people. Let people know what you need in order to thrive. Embrace those you feel drawn towards as positive people.
Activity: Making the best of me…
1: Ask yourself how others can get the best out of you
2: Offer what you can realistically do
3: Communicate what inhibits your productivity with others
4: Actively describe what you need from others in order to thrive
Tip 4:Express gratitude and forgiveness for enhanced wellbeing. Not always easy, but worth investing in. This task not only unburdens your mind, but allows you to see all of the good things currently going on in your life. Regularly write down 5 things that you are grateful for. Also…try to forgive yourself, and others…often.
Tip 5: Address your work life balance as a fluid entity. I believe that the idea of a separate home and work life is changing. This is a good thing. It takes the pressure off and allows you to be a whole person, rather than one split in two…See yourself as a whole being, a working, living and family centred being. You cannot slice yourself into pieces.
Living in the ‘now’ rather than being at either home or work also allows us to enjoy more of ourselves and our lives. Notice where you are, what you are doing…Smell the flowers, look around you as you move, work, play and just allow yourself to ‘be’.
Tip 6: Eat Sleep move, repeat. It really is that simple, but utterly essential for optimum productivity, stress reduction, health and wellbeing. Eat nutritious food regularly, sleep 7-8 hours a night and move…Exercise, walk, swim, run, cycle…Be outdoors as often as possible.
Tip 7: Write. Write your thoughts, your feelings, your ‘to do’ lists, your ideas, your goals down regularly. This not only means that they are out of your head, allowing your mind to be quieter, they are also made real…They are good to share..and worth addressing (when you feel able).
Tip 8: Talk about who you are. There is a tendency to talk about work first. What we do, what we are working on and what we are planning to work on. Start new conversations with how you enjoy your hobbies or your favourite music. This lets other people know that you are indeed human, and it also gives you an identity other than your work persona. Be authentic. It is healthy for you, and others to know the real and whole you. You are fab 🙂
Tip 9: Help other people and accept help yourself. Lift one another up, support colleagues, show gratitude, offer support and guidance where you can. Be a mentor. Be a positive role model. Be the change you want to see in the workplace and accept all of this in return. This will not only make you feel good, it will change the culture of your workplace, and bring about reciprocity for everyone’s success.
Tip 10: Celebrate the successes of yourself and others. Yes. Focus on the great things that you and your colleagues have achieved. However big or small, these feelings of success will snowball into a self fulfilling prophecy, where you feel valued, supported and part of a team that cares. Some people will feel uncomfortable about doing this, and feel icky when they see others wallow in their own brilliance. But what is the alternative? We all talk about how rubbish we all are? How will that make us feel?…
Spend time reflecting on what you have achieved. Write them down…use these achievements to inform your own vision of yourself…This is who you are. You are great.
As long as the feelings of celebration and success are reciprocated and directed towards others as well as yourself….Let the high fives roll.
I do hope that these tips will resonate with some academics looking for something new to try. In the spirit of sharing, please feel free to add more tips below.
You deserve to be happy – Until next time, look after yourselves and each other ❤💙💜





















 is needed!
is needed!